
Claudette M. Lajam, M.D., Assistant Professor of Orthopedic Surgery, NYU Hospital For Joint Disease
Dr. Claudette Lajam is an avid cyclist and athlete. She is a team physician for USA Cycling. She served on the Board of Directors of the New York Cycle Club and is a major sponsor of an amateur cycling race team. She cares for recreational and elite cyclists as well as endurance and other athletes.
Dr. Lajam is a Board Certified Orthopedic Surgeon with special interest in joint replacement, revision joint replacement, and sports medicine/arthroscopy. She performs total knee replacement, total hip replacement, arthroscopic ACL reconstruction and arthroscopic rotator cuff repair for the shoulder. Dr. Lajam is a host on The Orthopedic Show for SIRIUS/XM Doctor Radio. You can listen to her on Monday evenings from 6-8 pm, EST on SIRUS 114 or XM 119.
Knee pain is the most common lower extremity problem in cyclists. It can result in decreased participation, enjoyment and performance. Hip dysfunction can also cause significant pain and detriment to performance and enjoyment. While it is impossible to cover all types of pathology in this article, we will address the more common sources of pain. A vexing challenge in treatment of lower extremity pain is to identify the pain generator, or “PG.” Pain can be caused by systemic disease, lumbar spine issues, hip pathology, knee pathology, neurologic conditions and vascular conditions. It is important to seek out a physician who understands cycling and the unique stresses placed on the body when riding. It is also imperative that each cyclist have a primary physician who can monitor general health and who can provide pre-participation evaluation before periods of intense training or competition.
{kind=link}
Knee Pain
The knee takes on tremendous stress during cycling. With average cadence of 80 rpm, the knee performs thousands of repetitions of the singular pedaling motion. Most stress is undertaken in the patellofemoral compartment (the area under the kneecap). Injury to this area can result in pain and decreased performance. Remember that any inflammatory condition within the knee joint can cause a part of the quadriceps muscle to shut down, thus magnifying any muscle imbalances that have already occurred. It is important to heed warnings of pain and swelling in the knee with early treatment so that the problem does not become worse! Also, know that the PG for knee pain can be the hip or the lumbar spine. If pain in the knee is vague or seems to shoot into the groin or the back and does not go away with treatment, evaluation of the hip and spine is recommended.
- Chondromalacia of the patella: Chondromalacia means “bad cartilage.” It is characterized by changes in the joint surface cartilage on the undersurface of the patella, on the groove that the patella rides in, or in both areas. These changes can come from trauma, can be age-related or can occur because of natural alignment of the joint.
- Symptoms: pain behind the kneecap, swelling, catching (the knee gets stuck in the extended position and needs to be wiggled to bend). Pain precipitated by hilly rides, riding in bigger gears or at slow cadence. Pain also with stairclimbing or descent, squatting or deep knee bends.
- Diagnosis: the doctor will examine the knee for alignment (“Valgus” knees are more likely to have this condition), motion and telltale signs of the condition. Xrays are taken to view the joint spaces and to exclude fractures. Cycling history to determine bike fit, riding habits and injury history can help with diagnosis.
- Treatment: A period of lower resistance training (high cadence and flat terrain) along with anti-inflammatory medication, icing and muscle balancing exercises – including strengthening quadriceps and stretching IT Band, hamstring and calf muscles – is usually helpful. Cleat and saddle position should be checked to rule out fit issues. If the problem is purely anatomic, sometimes realignment surgery is an option.
- Patellar tendonitis: Inflammation of the tendon between the kneecap and the shin bone can be very painful and tough to treat.
- Symptoms: Pain when pedaling or extending the knee against resistance. Location is in the tendon and soft tissue just below the tip of the kneecap. There may be swelling of the tendon and tenderness to the touch.
- Diagnosis: Physical examination shows swelling and tenderness in these locations. Xrays are usually negative. MRI will show inflammation of the tendon and the absence of other pathology.
- Treatment: Bike fit is very important. Cleat and saddle position should be checked to see if too much lateral stress is being placed on the tendon. Training modification to flat terrain and low resistance riding is recommended until pain-free. Focused icing and NSAID medication is helpful to reduce inflammation. Formal physiotherapy can assist. Injections with steroids are NOT recommended. This condition is very frustrating and may take a long time to treat.
- Meniscal or ligamentous tears: Internal pathology of the joint can occur in all age groups. In younger athletes, twisting injury or trauma is usually involved. In older patients, degenerative meniscal tears can cause irritation within the joint and start a cascade of events that can affect performance.
- Symptoms: Meniscal tears can cause swelling, locking in a flexed position and catching of the knee. Pain is usually on the inside or the outside of the knee. Ligament tears cause instability and difficulty doing cutting or twisting motions.
- Diagnosis: Physical examination alone can give a lot of information. Xrays to rule out fractures or arthritis are performed. If conservative treatment fails or if ligament tears are suspected, an MRI may be ordered to see the soft tissues.
- Treatment: Most meniscal tears in older people can be treated non-surgically. If this fails and MRI shows significant tears, arthroscopic surgery can be helpful. Ligament tears are treated according to the particular needs of the patient. Many cyclists who are older elect not to have ACL reconstruction, as cycling does not involve cutting and twisting. Younger patients will usually elect to have ACL reconstruction so as to decrease instability and perhaps delay onset of arthritis in the joint.
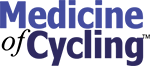
- Iliotibial band syndrome: results from friction of the expansion of the Iliotibial band (ITB) on the outside of the femur bone during repetitive motion. The band moves from anterior to posterior during pedal motion. When inflamed, it can cause severe pain on the outside of the knee.
- Symptoms: Pain on the outside of the knee, often stabbing or burning, that occurs in concert with the pedal stroke. There may also be pain at the outside flare of the hip and down the lateral thigh to the outside of the shin bone. Pain goes away with rest early on, but with increasing severity there is pain all the time.
- Diagnosis: physical examination is the key. Tenderness, positive Ober test for tightness of the ITB and sometimes even snapping of the band along the condyle. MRI has limited utility here, but is performed sometimes to rule out other confounding conditions.
- Treatment: nonsurgical treatment is useful in most cases. Bike fit should be examined, particularly cleat positioned too internally rotated or too forward on the shoe. Cleats with too little float can also exacerbate this condition. Focused stretching, cross-fiber ice massage, rest and NSAID are helpful. Foam roller stretching of the ITB can help prevent the condition from returning. Surgery to release the posterior fibers of the band can be performed in the most stubborn cases.
- Plica syndrome: The normal knee is enclosed in a capsule of tissue. When this capsule becomes inflamed, sometimes folds or shelves of the capsule become a mechanical source of pain in the knee. These folds are called “plica,” which means “fold.”
a. Symptoms: Pain, swelling and mechanical clicking, usually on the inside of the knee. Pain is brought on by motion and improves at rest.
b. Diagnosis: Physical examination is important, since on MRI the plica may appear as normal capsule.
c. Treatment: Elimination of inflammation is the key to treatment. NSAID medication, focused icing and training modification to exclude painful activity are the best treatment. Surgical treatment with arthroscopy can remove persistent plica.
{kind=link}
Hip Pain
The hip is increasingly recognized as a source of pain in athletes. Improvements in understanding of the joint, along with advances in technology have allowed better surgical treatment of early problems. Again, the PG for hip pain may be a lumbar spine condition. If hip pain is unexplained by thorough evaluation, a lumbar spine evaluation is recommended.
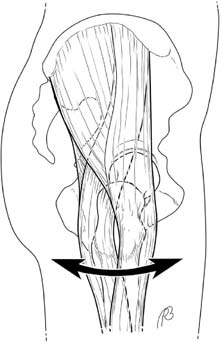
- Snapping hip syndrome: When snapping is painless it does not require treatment. For painful snapping, there are two types: Internal and External. Internal snapping is caused by the iliopsoas tendon’s sliding over the front of the femur during movement of the hip, particularly during a “frog kick” type of movement. External snapping is caused by the upper portion of the Iliotibial band when it passes over the greater trochanter of the femur.
- Symptoms: For internal, the athlete may have deep groin pain and will experience a snap when the hip is moved in a frog kick type of motion. The snap sometimes can be heard across the room. For external, the athlete may believe that the hip is “dislocating.” The outer edge of the hip can be seen to push out during motion and then come back in. Pain is over the outside of the hip.
- Diagnosis: Internal snapping can be tough to diagnose. Physical examination is the key, along with imaging studies to rule out other issues. Bursography, which involves the injection of contrast into the bursa, can be of value in certain cases. External snapping is also diagnosed with physical examination and imaging to rule out other causes if necessary. It is very important to establish an accurate diagnosis before undergoing any surgery.
- Treatment: For internal snapping, an intensive stretching program focused on the lower back and hip is recommended. NSAID treatment and modification of training to exclude painful activities is important until pain is gone. Core strengthening can be helpful. For external snapping, modification of training and treatment of inflammation are key. Strengthening of abductors and the foam roller may be helpful in decreasing snapping. Surgical treatment for persistent internal snapping involves release of part of the tendon from the lesser trochanter of the hip. This can now be performed arthroscopically, but only after other measures have failed.
- Impingement Syndrome: Abutment of the bones in the hip can cause pain and dysfunction. When the cycling pedal stroke causes this event, pain and limitation of performance can occur.
- Symptoms: Persistent pain in the groin area, brought on by flexion and usually internal rotation of the hip.
- Diagnosis: Physical examination and plain X-rays to rule out other issues are important first steps. MRI is helpful if an associated soft tissue lesion is suspected. Diagnosis is tricky as there are many PGs within the hip joint.
- Treatment: Modification of activity, a stretching program and anti-inflammatory medication can be helpful. Bike fit should be assessed to ensure there is no excessive hip flexion during pedal stroke. When pain is persistent, surgical treatment with arthroscopy and removal of the impinging part of the bone can be performed. Recovery from surgery takes 6-12 weeks, depending on the procedures performed.
- Labral tears: The soft tissue rim around the hip socket is called the labrum. When tears occur, the loose piece may flip in and out of the joint and cause inflammation and pain. Tears are also thought to cause loss of the suction effect of the joint, thus creating micro-instability.
- Symptoms: Groin pain with motion, especially when the hip is brought into flexion. The athlete may feel a click or catch inside the hip. The athlete can sometimes remember a traumatic event after which the pain began.
- Diagnosis: Can be difficult, but combination of physical examination, x-rays and MRI with contrast can show the lesion.
- Treatment: Early treatment includes training modification, stretching and NSAID medication. If this fails and a labral tear is seen, the athlete may elect for surgical treatment with arthroscopic repair or debridement. If surgery is performed, it is important that the surgeon address any bony impingement. Recovery from surgery is 6-12 weeks.
- Arthritis: When the bearing surface cartilage wears away, athletes may feel pain and stiffness in the hip.
- Symptoms: Pain and stiffness in the groin and hip. Pain occurs with weight bearing. The athlete may limp on the affected side. Cycling might not be painful, even with severe disease.
- Diagnosis: Plain x-rays along with history and physical examination will show arthritis in the hip. MRI is generally not needed if x-rays show the condition.
- Treatment: Conservative treatment includes NSAID medication, stretching and core strengthening. Cycling can continue so long as the athlete can tolerate it. Fit may need to be adjusted so that the stiffness in the hip does not affect the other joints and the low back. This can be done by raising the handlebar position to more upright. Arthroplasty hip surgery is the only reliable surgical treatment. Hip resurfacing or replacement may be performed depending on the severity.
- Fractures: Traumatic fractures of the hip can occur after crashes or trauma. These are fairly obvious and should be treated immediately. However, stress fractures of the femoral neck can occur over time and are more difficult to diagnose. Catastrophic consequences may occur if a stress fracture becomes a complete fracture in a young person. Many cyclists have low bone mineral density from lack of weight bearing activity and are at risk.
- Symptoms: Groin pain, mostly with weight bearing activity and sometimes at rest. Pain may be vague. This condition may also present as vague anterior knee pain or thigh pain.
- Diagnosis: Evaluation and plain x-rays may not show the fracture. If pain is persistent and not explained by examination, MRI should be performed to rule out stress fracture.
- Treatment: Depending on location of the fracture, surgery may be indicated to place screws across the area so as to prevent completion of the fracture. Some types of fractures can be treated conservatively with protected weight bearing and modification of activity. If stress fractures are seen in young athletes, assessment of bone mineral density and evaluation by a general doctor is recommended to rule out other conditions.
Conclusions
Lower extremity pain is common in cyclists, but many conditions can be treated conservatively. It is important to recognize these issues and treat them early so that they do not affect performance long-term. Bike fit is critical in prevention and minimization of lower extremity pain. Most athletes can continue cycling at low intensity during treatment and recovery from injury.
Comments are closed.